
By Joanna Lane with comment from Dr Charles Shepherd
I don’t have ME, but I have something important to say that I hope may help people who have.
Twelve years ago, our 31-year-old son Christopher killed himself. We were devastated and desperate to find reasons. We wondered about the serious head injury he’d had when he was seven and we found that head injury survivors are between twice and four times more likely to commit suicide than other people (1).
The more we researched head injury the more we found out. One common complication of head injury is hypopituitarism, when the pituitary gland is damaged and does not make some, or all, of the hormones the body needs to work properly (2).
Looking back, we recognised some of the symptoms in Chris. For example, depression, impotence (which we only knew about after his death) and something wrong with his body thermostat, because he seemed to have an aversion to heat.
Dr Charles Shepherd, Hon. Medical Adviser, ME Association:
“When a GP or specialist considers a patient’s symptoms and medical history prior to making a diagnosis of ME/CFS there are a number of common and less common conditions that should always be considered, tested for and excluded.
“Hypopituitarism is a rarely diagnosed brain disease that can cause fatigue and some of the other symptoms that we see in ME/CFS. Unfortunately, it is not a condition that general practitioners are used to dealing with – so it is sometimes missed and can result in an incorrect diagnosis.
“It is caused by damage to the pituitary gland – a small pea-sized gland in the brain that controls the output of various hormones in the body. These include thyroxine (from the thyroid gland), cortisol (from the adrenal glands), growth hormone, sex hormones and antidiuretic hormone. As a result, there is a decrease in the amount of some or all of hormones that it controls.
“The most common cause of hypopituitarism is a tumour in the pituitary gland. Other causes include brain infections, surgery and radiotherapy to the brain, trauma to the brain, drugs, and autoimmune disease. Studies suggest that between 20 and 30 per cent of people who have a serious head injury also suffer damage to the pituitary gland.
“Symptoms can appear suddenly or gradually over time and will depend on which hormones are being affected and the degree of deficiency.
“They can include fatigue, muscle weakness and headaches; weight loss and low blood pressure (from low cortisol); male impotence or irregular menstrual cycles (from low sex hormones), dry skin, weight gain and cold intolerance (from low thyroid hormone)and increased thirst and urination (from decreased antidiuretic hormone).
“Measuring the levels of the various hormones, visual field tests and neuroradiology investigations should be carried out where a pituitary gland problem is suspected, as well as hormone stimulation tests in some cases .
“Treatment of hypopituitarism will involve life-long replacement therapy of all the hormones that are not being produced in normal amounts.
“If you have suffered a head injury and/or recognise the symptoms associated with hypopituitarism and have not had your hormone levels checked recently, this is something to discuss with your GP.”
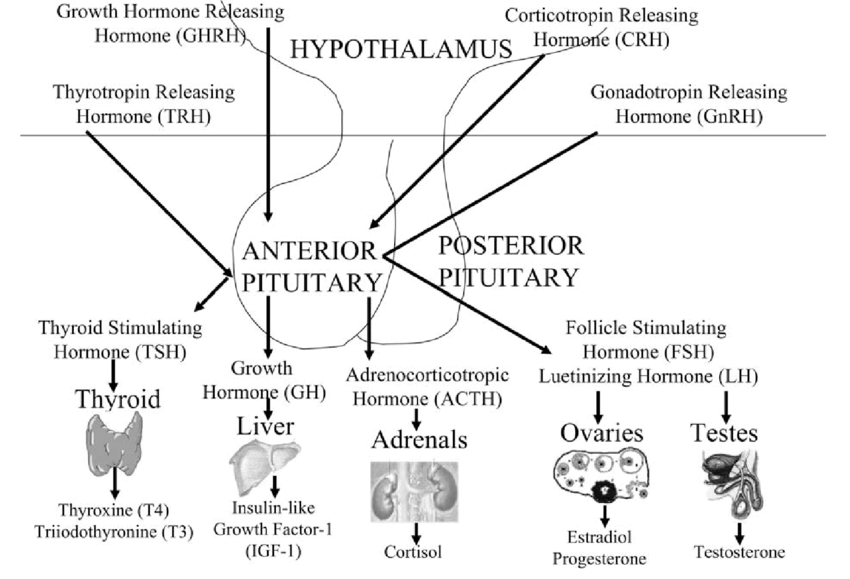
The pituitary gland and hormone production
Source: Derr et al. Pre-Analytic Considerations for the Proper Assessment of Hormones of the Hypothalamic-Pituitary Axis in Epidemiological Research (2006)
More information:
- MEA Free Leaflet: ME/CFS & The Importance of Early and Accurate Diagnosis
- MEA Clinical and Research Guide: Differential Diagnosis & Testing
Missed diagnosis?
It seemed as though nobody knew about these risks. When I started to try to raise awareness, people with hypopituitarism wrote to me. I soon learned that many of them had been misdiagnosed with ME/CFS on the way.
This is not surprising because when you consider ME/CFS symptoms and compare them with the Pituitary Foundation’s list for hypopituitarism there is a surprisingly large overlap. For example, the hypopituitarism symptoms include many which the ME/CFS community will recognise only too well:
Fatigue, loss of libido, muscle wasting, pale skin, weight loss or gain, and POTS (with its accompanying sleep abnormalities, headaches, dizziness, exercise intolerance and tinnitus). I should mention here that most hypopituitarism sufferers will have only a selection of these symptoms, because out of the five major pituitary hormones not all may be affected.
What the people who wrote to me with their stories (3) had in common was that they were persistent, and independent-minded enough not to accept their ME/CFS diagnosis unquestioningly.
They looked up their symptoms. They also had the money, usually, to finance private testing – testing which their GP was often reluctant to give them, partly because it is expensive, partly because they are not trained to diagnose hypopituitarism.
I began to suspect that these tenacious people were the tip of the iceberg, and that possibly many thousands in the ME/CFS community have been misdiagnosed. Maybe they don’t have ME/CFS at all, but hypopituitarism? Perhaps they can have hormone replacement treatment and get their lives back? How wonderful that would be?!
- Joanna Lane has written on this subject for the Daily Mail in 2014 in an article that includes people who were misdiagnosed with ME/CFS
The data
My suspicion hardened to near certainty when I looked at the numbers. Post-Traumatic Hypopituitarism (PTHP) happens to 50 people in every 100,000 annually (4). This means 33,000 cases every year in the UK.
Up until 1986 only a handful of cases were reported, and since then the number of diagnoses has crept up slowly until now it is around 20,000 a year – still over a third short of what it should be.
After decades of under-diagnosis, there could be up to a million invisible cases of PTHP in the UK today, which is the figure suggested in BBC’s Inside Health programme eight years ago (5).
Even this huge figure is not the whole story, because serious head injury is not the only cause of hypopituitarism. Other possible causes are concussion, pituitary tumours, radiation of the head, brain surgery, auto-immune disease, infections or inflammatory diseases of the brain, and some medications (6).
What has happened to these very sick people? Could they have been misdiagnosed with ME/CFS?
What to do next
My message is: research your symptoms, research hypopituitarism, and if you think there’s a match, ask for the right diagnostic tests. If you have ever had a head injury or concussion, even long ago, do it straightaway!
The brain injury charity, Headway, has a page about ‘Hormonal Imbalances’ (7) which you can show your GP. Otherwise, you can show them print-outs from the Pituitary Foundation and the Mayo Clinic website, marking the symptoms on their list that you believe might apply.
My husband, my daughter and I have set up a charity, Christopher Lane Trust, which gives information about diagnostic tests, including information about the unreliable tests that are sometimes used to exclude hypopituitarism, and we may even be able to fund private testing for people whose GPs will not authorise the correct tests on the NHS.
I wish everyone who goes down this road good luck – and persistence!
References:
(1) Suicide after traumatic brain injury: a population study, J Neurology, Neurosurgery, and Psychiatry 2001
(2) Schneider HJ et al, Hypothalamopituitary Dysfunction Following Traumatic Brain Injury and Aneurysmal Subarachnoid Haemorrhage: A Systematic Review, 2007, JAMA:
(3) For example from the BMJ:
Example 1
Example 2
Example 3
(4) Fernandez-Rodriguez E et al, Hypopituitarism following traumatic brain injury: determining factors for diagnosis, Front Endocrinol 25 August 2011 doi: 10.3389/fendo.2011.00025
(5) BBC Inside Health Podcast 09 April 2013: Transcript
(7) Headway: