
What are ME/CFS and Long COVID?
ME/CFS (myalgic encephalomyelitis / chronic fatigue syndrome) is a complex, long-term condition that affects multiple body systems and varies greatly from person to person. Its cause is not fully understood, although it often develops after an infection, its pathophysiology is still being investigated. Symptoms commonly include profound fatigue that is not relieved by rest, post-exertional worsening of symptoms, brain fog, sleep problems, flu-like feelings, pain, headaches, digestive issues, nausea, and sensitivity to light and sound.
Long COVID is increasingly recognised as a post‑viral fatigue syndrome triggered by SARS‑CoV‑2 and often shares the same symptom clusters as ME/CFS. Both conditions can cause long‑term, fluctuating symptoms and major disruption to daily life.
A significant proportion of people with Long Covid also experience a distinct layer of symptoms tied directly to organ involvement during the original infection — affecting the lungs, heart and blood vessels, liver, kidneys, brain and nervous system, gastrointestinal tract, or skin — where the infection caused lasting damage or disrupted normal function. This marks a key difference between the two conditions.
ME/CFS has long been recognised as a post‑viral fatigue syndrome and neurological condition by the World Health Organization, NHS and Department of Health.
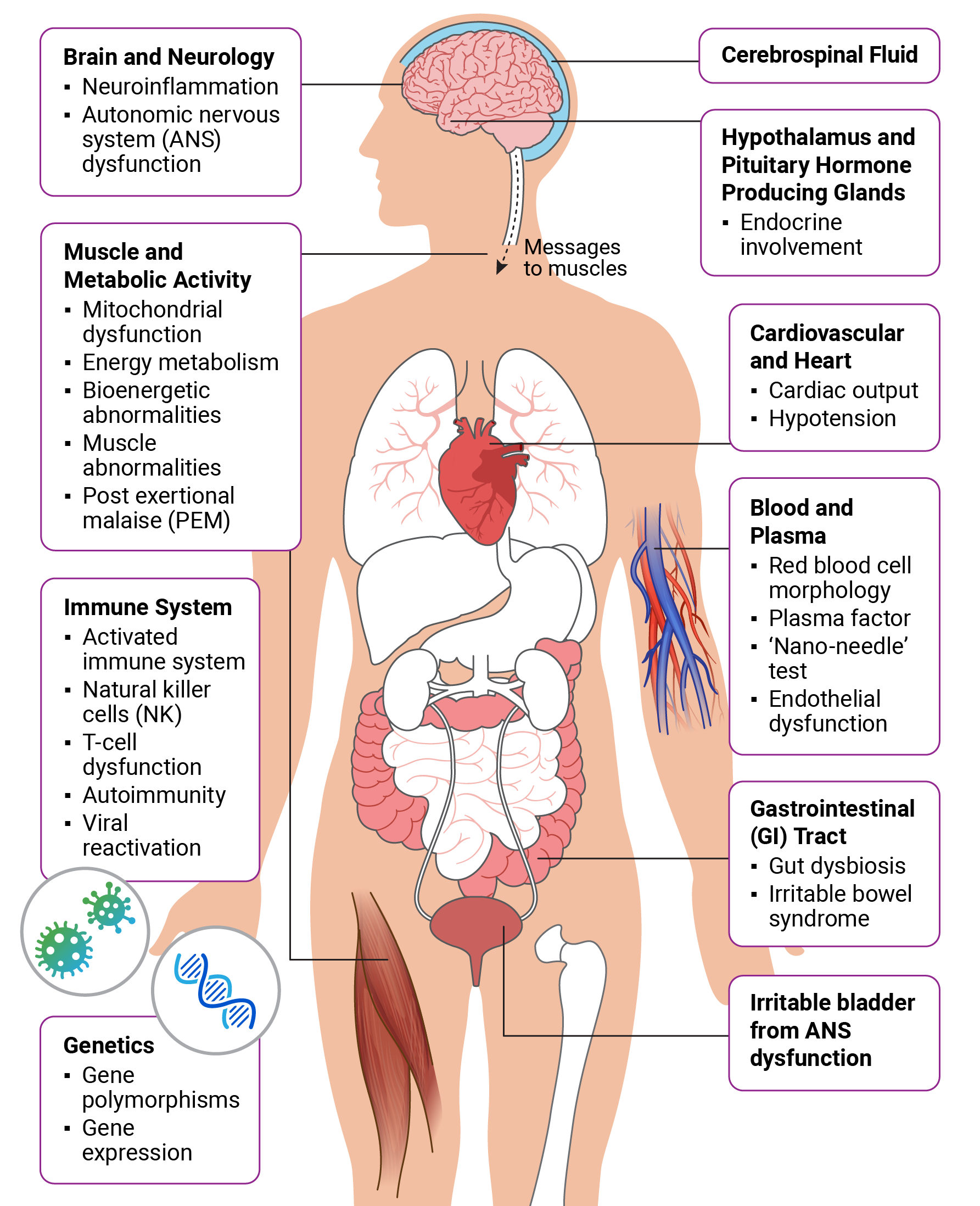
ME/CFS is a multi-systemic illness meaning it affects multiple systems in the body. The diagram shows areas where research has found levels of dysfunction. More information in symptoms section below.
Symptoms
ME/CFS Core Symptoms
Profound Fatigue
not relieved by rest and that significantly reduces daily functioning
Post Exertional Malaise (PEM)
activity causes delayed, disproportionate worsening and prolonged recovery (hours to weeks)
Unfreshing Sleep
or disturbed sleep
Cognitive Difficulties
“brain fog”: slowed thinking, memory and concentration problems
Common symptoms in ME/CFS and Long COVID

Orthostatic Intolerance
and autonomic dysfunction, including dizziness, palpitations, fainting, nausea on standing or sitting upright from a reclining position
Temperature Sensitivity
resulting in profuse sweating, chills, hot flushes, or feeling very cold
Flu Symptoms
including sore throat, tender glands, nausea, chills or muscle aches

Neuromuscular symptoms
including twitching and myoclonic jerks

Pain
including pain on touch, myalgia, headaches, eye pain, abdominal pain or joint pain without acute redness, swelling or effusion
Sensory Sensitivities
including to light, sound, touch, taste and smell

Gastrointestinal Problems
Abdominal pain and diarrhoea, irritable bowel syndrome, or an inflammatory bowel syndrome
Alcohol intolerance
or intolerance to certain foods and chemicals
Common Long COVID-specific symptoms
Cardiac symptoms
heart-rhythm disturbances / cardiac arrhythmias and palpitations on exertion
Respiratory
shortness of breath and/or cough, chest pains
Loss of Smell or Taste
Rash
Skin rashes – including ‘Covid toe’
Hair loss
Symptoms commonly fluctuate and vary widely between people.
Diagnosis
- A diagnosis of ME/CFS can be made in children, young people, or adults who have experienced the core symptoms listed above for at least 3 months, provided no other condition explains them. Long Covid, by contrast, refers to symptoms that persist beyond 4 weeks after acute COVID-19 — particularly beyond 12 weeks — once other possible causes have been ruled out.
Referral
- Adults should be referred directly to a specialist ME/CFS team to confirm diagnosis and put together a care and support plan. Children and young people should first be assessed by a paediatrician, then referred to a paediatric ME/CFS specialist team where appropriate.
(Please note: funding and commissioning for ME/CFS and Long Covid services vary considerably across the country. In many areas, services for the two conditions have merged, offering combined pathways. Elsewhere, dedicated services may not exist at all, meaning referrals are made based on specific symptoms instead — for example, to a respiratory consultant for breathlessness, or to cardiologist for POTS/orthostatic intolerance. In most areas, a GP referral is required, and your GP should carry out the blood tests set out in the NICE 2021 guidance before making it.)
More about ME/CFS and Long COVID can be found in our booklets:



NICE Guidance
The National Institute for Health and Care Excellence (NICE) publishes evidence‑based guidance for both ME/CFS and Long Covid.
The ME Association endorses the NICE ME/CFS guideline and recommends patients, families and carers read it and discuss recommendations with healthcare professionals.
The NICE Guideline on ME/CFS covers illness severities, principles of care, diagnosis, specialist services, symptom management, multidisciplinary care, safeguarding, work and education, and care for severe / very severe ME/CFS.
The NICE Rapid Guideline on Long Covid covers identification, assessment, investigations, referral, planning care, self‑management, multidisciplinary rehabilitation and service organisation.
Severity
Severity ranges from mild (reduced activity but largely independent) to very severe (bedbound, dependent on care). Around a quarter of people with ME/CFS have severe disease. The condition has substantial personal, social and economic consequences, many people experience delays in diagnosis and unequal access to specialist services.
Definitions of severity are not clear cut because individual symptoms vary widely in severity and people may have some symptoms more severely than others. The definitions below provide a guide to the level of impact of symptoms on everyday functioning. Source: The 2021 NICE Guideline on ME/CFS

Mild
Self-care and light domestic tasks are usually manageable, sometimes with support, though mobility can be difficult. Most people at this level continue working or studying, full or part time, but only by giving up leisure activities and social life entirely. Days off and weekends are often needed just to cope with the week ahead.
Moderate
Mobility is reduced and daily activities are restricted across the board, though symptoms and ability can fluctuate between better and worse periods. Work or education has usually had to stop, and regular rest is essential, often including time lying down in the afternoon. Nighttime sleep tends to be poor and disturbed.
Severe
Only minimal daily tasks are possible, such as washing the face or brushing teeth. Significant cognitive difficulties are common, and a wheelchair may be needed for mobility. Leaving the house is often impossible, or triggers a severe, prolonged crash afterward. Much of the day may be spent in bed, with heightened sensitivity to light and sound.
Very Severe
Bed rest is constant, with full dependence on others for care. Help is needed with personal hygiene and eating, and sensory stimuli are hard to tolerate. Some people cannot swallow and require tube feeding.
Treatment
There is currently no universally effective drug treatment for ME/CFS or Long Covid. Research and clinical trials are ongoing. Care should be personalised and multidisciplinary, aiming to stabilise symptoms, reduce harm and improve quality of life.
Key treatment elements include:
Early and accurate diagnosis
Pacing to avoid PEM (Post Exertional Malaise)
Pace activity to reduce energy crashes
Tailored symptom management (sleep, pain, orthostatic symptoms)
It can help to keep a symptom diary (triggers, activity, recovery)
Occupational, social and psychological support where needed
Timely access to specialist services
Discuss referral options with your GP
Seek medical advice if symptoms persist or worsen after an infection to rule out other causes and discuss referral. Urgent assessment is required for signs of acute or life‑threatening complications or severe psychiatric risk.



More information
Further reading for information and guidance



Free Literature Library
Written by Dr Charles Shepherd, other advisers and topic experts
Information for Healthcare Professionals
If you are a healthcare professional searching for further information about ME/CFS, the ME Association provides free information on the diagnosis and management of ME/CFS, and can direct you towards further learning resources.
