
Charlotte Rawlinson, ME Association Deputy Manager of Health and Social Care
SNOMED CT (Systematised Nomenclature of Medicine – Clinical Terms) is an internationally validated system to record clinical information in the patient record and aids in enhancing communication and interoperability of clinical data across healthcare systems.1 This article explores the role of clinical coding in improving care for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Long COVID (LC) patients.
SNOMED CT Coding of ME/CFS and LC
Through engagement with specialist service leads, the ME Association (MEA) Health and Social Care (HASC) team has encountered reports of inconsistent coding of ME/CFS and LC being applied to electronic medical records.2 Inadequate or inaccurate data of this nature may have far-reaching consequences as it hinders specialist service planning and results in missed research opportunities. Concerns about the unsatisfactory coding of ME/CFS have been formally raised with the All-Party Parliamentary Group (APPG) on ME, as well as with the Department of Health and Social Care (DHSC) and NHS England, during discussions on the ME/CFS Delivery Plan.3
SNOMED CT currently categorises ME/CFS under the Fully Specified Name (FSN) ‘Chronic fatigue syndrome (disorder)’ (SCTID: 52702003). However, clinicians may use a range of acceptable terms listed in the NHS Digital SNOMED CT Browser including ‘ME/CFS – myalgic encephalomyelitis/chronic fatigue syndrome’ which is listed as a preferred term4 and aligns with the terminology used in the latest NICE guidance (NG206).5
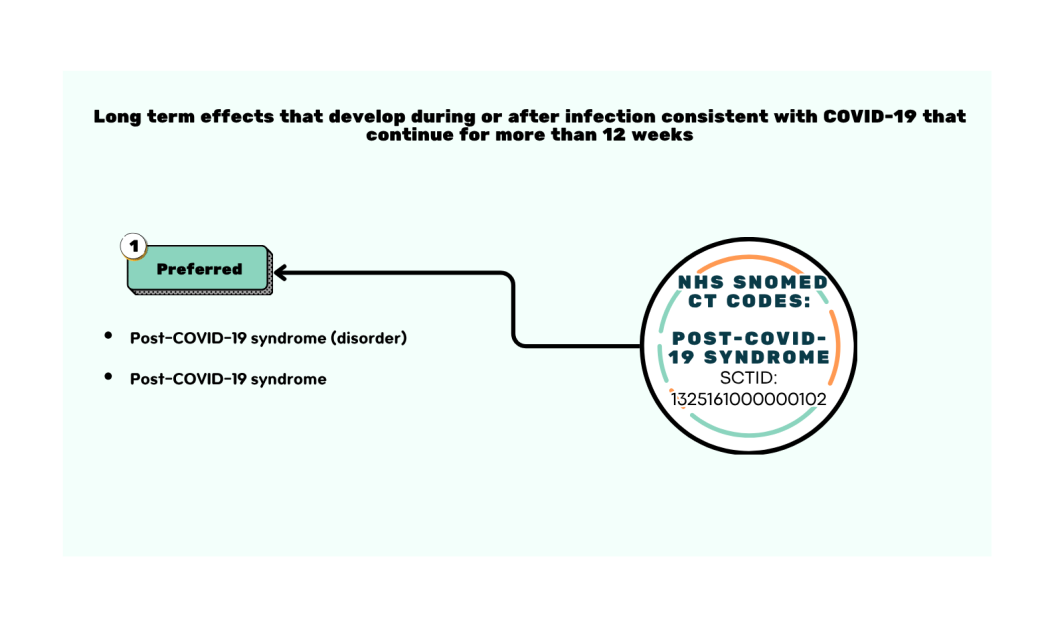
SNOMED CT also permits more detailed coding such as illness severity, symptoms and co-morbid conditions. The additional insight this data may provide could identify and facilitate potential areas of research such as prognosis, common disease progression patterns and co-morbid conditions including hypermobility6 and postural orthostatic tachycardia syndrome (POTS).5 NICE categorisation of LC includes both ongoing symptomatic COVID-19 (from 4-12 weeks) and post-COVID-19 syndrome (12 weeks or more).7 Ongoing symptomatic COVID-19 is classified under the FSN ‘Ongoing symptomatic disease caused by severe acute respiratory syndrome coronavirus 2 (disorder)’ (SCTID: 1325181000000106).8 The FSN for post COVID syndrome is ‘post-COVID-19 syndrome (disorder)’ (SCTID: 1325161000000102).9

The Importance of Coding
Effective clinical coding facilitates audits, supports research and improves communication across healthcare settings.10 The latter is especially important in the coordination of care for patients with conditions such as ME/CFS and LC which are associated with symptoms spanning multiple organ systems and, therefore, may require input across multiple care settings and specialities.
On a larger scale, clinical coding also supports epidemiological studies and strategic allocation of health resources.10 Prevalence estimates of ME/CFS and LC vary greatly and a comprehensive UK epidemiology study is long overdue.11 Furthermore, resource allocation for specialist services is heavily dependent on referral numbers and local prevalence data. The use of SNOMED CT coding for ME/CFS and LC in national health databases facilitates large-scale epidemiological data which allows for more targeted public health interventions and resource allocation.
LC research is a newly emerging field and biomedical research into ME/CFS has been historically underfunded and is recognised as being one of the lowest-funded diseases, relative to disease burden, by the US National Institutes of Health (NIH).12 The epidemiological data generated by national coding efforts has the potential to influence biomedical research funding which is especially important for diseases such as ME/ CFS where the underlying pathophysiology has not yet been fully elucidated and historically patients have faced challenges arising from disbelief and lack of validation of their condition within the medical profession.5
The Path Forward: Improving ME/CFS and LC Coding in Clinical Practice
All NHS healthcare providers in England must use SNOMED CT for capturing clinical information and have a role in ensuring conditions are accurately coded.1 The cost of effecting improvements in clinical coding might include education and training of healthcare providers. However, this may be partially offset by incidental savings. One NHS hospital found that adopting SNOMED CT data entry lists (subsets) resulted in significant annual cost savings owing to improved scheduling and resource allocation.13 Resultant benefits would be expected in the areas of diagnosis, patient management, epidemiological monitoring and research into the underlying pathophysiology of ME/CFS and LC. Technological advances, including artificial intelligence tools, make this an opportune time to ensure the accuracy of clinical coding data which has the potential to be analysed more quickly and cost-effectively than ever before, yielding valuable insights into these complex conditions.
The MEA HASC team will continue to advocate for accurate SNOMED CT coding of ME/CFS and LC to Integrated Care Boards, Health Boards, and primary and secondary care settings.
Charlotte Rawlinson
ME Association Deputy Manager of Health and Social Care

Published 5 June 2025; Last updated 1 Oct 2025
Disclaimer: The choice of SNOMED CT codes to be inputted into NHS clinical systems is a clinical decision. All released codes are available to be used in patient records as appropriate.
The above article was recently published in our magazine, ME Medical, a free quarterly magazine for healthcare professionals. If you are a healthcare professional who would like to sign up to receive a copy, or if you would like to nominate your GP to receive a copy, you can sign up here.
References:
- NHS England (2023). Clinical coding – SNOMED CT. v 1.2. [Accessed: 27 January 2025]. ↩︎
- ME Association (2024). Parliamentary question: ME/CFS: SNOMED CT Classification System in Primary Care. [Accessed: 27 January 2025]. ↩︎
- ME Association (2024). Medical Matters > Nomenclature: ME/CFS. [Accessed: 3 February 2025]. ↩︎
- NHS Digital (2025). Chronic fatigue syndrome (disorder). [Accessed: 27 January 2025]. ↩︎
- NICE (2021). Myalgic Encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: Diagnosis and management: Guidance. [Accessed: 27 January 2025]. ↩︎
- The ME Association (2024) Medical Matters: Hypermobility & ehlers danlos syndrome. [Accessed: 30 January 2025]. ↩︎
- NICE (2022). CKS Longterm effects of coronavirus (long COVID). [Accessed: 27 January 2025]. ↩︎
- NHS Digital (2025). Ongoing symptomatic disease caused by severe acute respiratory syndrome coronavirus 2 (disorder). [Accessed 27 January 2025]. ↩︎
- NHS Digital (2025). Post-COVID-19 syndrome (disorder). [Accessed 1 October 2025]. ↩︎
- Blundell, J. (2023) ‘Health Information and the importance of clinical coding’, Anaesthesia & Intensive Care Medicine, 24(2), pp. 96–98. doi:10.1016/j.mpaic.2022.12.006 ↩︎
- ME Association (2024). Prevalence: How many people have ME/CFS in the UK?, The ME Association. [Accessed: 29 January 2025]. ↩︎
- Mirin, A.A., Dimmock, M.E. and Jason, L.A. (2020) ‘Research update: The relation between ME/CFS disease burden and research funding in the USA’, Work, 66(2), pp. 277–282. doi:10.3233/wor-203173. ↩︎
- Jones, M. (2022). ‘Benefits of using SNOMED CT in the UK National Health Service (NHS)’, Roadmap to Successful Digital Health Ecosystems, pp. 489–497.doi:10.1016/b978-0-12-823413-6.00023-9. ↩︎