
One of the nation’s premier medical advisory organizations has weighed in on Long Covid with a 265-page report that recognizes the seriousness and persistence of the condition for millions of Americans. The National Academies said the condition could involve up to 200 symptoms, make it difficult for people to work and last for months or years.
“The significant overlap in clinical presentation between Long Covid and ME/CFS and FM raises the question of common mechanisms that could be involved in the pathogenesis of these conditions and offers the potential to use past clinical and biomedical research to accelerate the understanding of pathomechanisms specific to Long Covid.”
National Academies: Long-term Health Effects of Covid-19: Chapter 5.
Article extracts
By Pam Belluck, New York Times, 05 June 2024.
Diagnosis and consequences
There is still no standardized way to diagnose the condition and no definitive treatments to cure it. “There is no one-size-fits-all approach to rehabilitation, and each individual will need a program tailored to their complex needs,” the National Academies said, advising that doctors should not require patients to have a positive coronavirus test to be diagnosed with Long Covid.
The report said that some of the most troublesome symptoms — like brain fog and chronic fatigue — can prevent people from returning to work and should make them eligible for disability payments, though their symptoms may not fit the Social Security Administration’s current disability categories.
“Long Covid can result in the inability to return to work (or school for children and adolescents), poor quality of life, diminished ability to perform activities of daily living, and decreased physical and cognitive function for six months to two years or longer,” the report said.
Recovery from Long Covid
Some people recover with time, and there’s some evidence that after a year, many people’s symptoms have diminished. But some research suggests that recovery slows down or plateaus after that first year, the report said.
Because Long Covid varies so widely from person to person and affects so many body systems, each case must be approached individually.
For some people, “returning to work too early may result in health deterioration, and a gradual return to work plan may be advised,” the report said, especially for people with post-exertional malaise, a symptom that involves depleted energy or setbacks after doing activities that involve physical or mental exertion.
Employers may need to offer accommodations to returning employees, like allowing them to take frequent breaks or work remotely.
National Acadamies Report Extract
Chapter 5: Chronic Conditions Similar to Long Covid
While Long Covid has recently garnered significant attention because of its wide-ranging effects on a considerable portion of the global population, infection-associated chronic conditions (IACCs) are not a new phenomenon. Additionally, Long Covid shares many features with other complex multisystem chronic conditions, including myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and fibromyalgia (FM).
SARS-CoV-2 is the viral trigger for Long Covid. It is also hypothesized to be one potential viral trigger for ME/CFS and FM. Other mechanistic links have been suggested among these conditions, including abnormalities involving the immune system, central and autonomic nervous systems, cardiopulmonary system, gut microbiome, and energy metabolism. Additionally, given their common symptoms, treatments for ME/CFS and FM can help inform treatment for Long Covid.
Shared symptoms
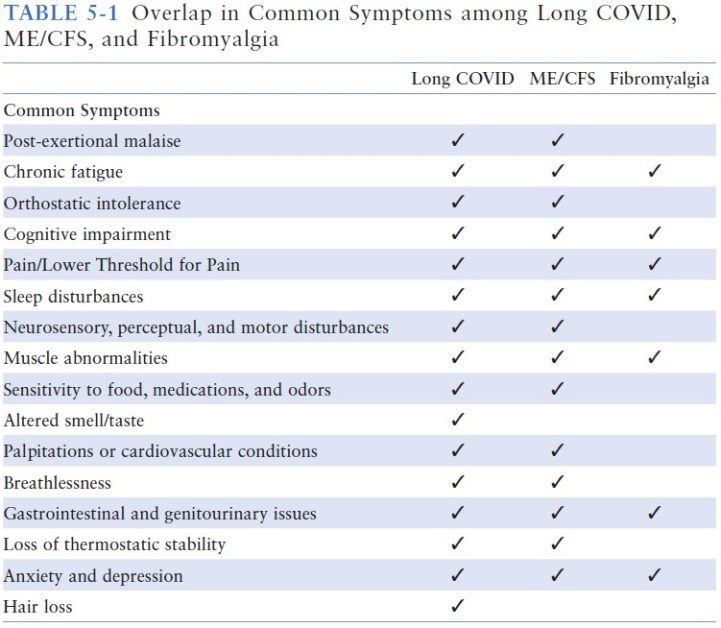
Systemic postinfectious syndromes share several symptom profiles, including post-exertional malaise, chronic fatigue, impaired concentration and memory, pain, and sleep disturbances (Jason et al., 2023).
Interestingly, the IOM (2015) core criteria for ME/CFS noted above are also core symptoms of Long Covid, as described in Chapter 3 of this report.
Komaroff and Lipkin (2023) provide a helpful table summarizing the overlap in clinical presentation between Long Covid and ME/CFS, based on the work of Wong and Weitzer (2021). The committee adapted this table to include symptoms of FM (Table 5-1).
Functional Implications
People with Long Covid, ME/CFS, and FM have decreased quality of life, including reduced physical and cognitive capacity, impairment in work performance, and reduced participation in society. In a study by Haider and colleagues (2023), individuals with Long Covid, ME/CFS, and FM reported a similar impact on physical and cognitive function; however, individuals with Long Covid versus those with the other two conditions reported lower pain and fatigue.
Other studies suggest that the functional impairment in people with ME/CFS may be greater than in those with Long Covid (Komaroff and Lipkin, 2023). A comorbid diagnosis of Long Covid with ME/CFS and/or FM further exacerbated pain, fatigue, and psychological domains compared with Long Covid alone (Haider et al., 2023).
Data currently under review show that ME/CFS and Long Covid cohorts do not differ significantly in any domain of quality of life using either the 36-Item Short Form Survey (SF-36) or the World Health Organization Disability Assessment Schedule (WHODAS) (Figure 5-1), the Hospital Anxiety and Depression Scale (HADS), or the Modified Fatigue Impact Scale (MFIS).
For all three chronic conditions, symptoms are cyclic, with some relatively “good” days and frequent “bad” days. Some people with the conditions are able to perform their responsibilities at home and work, while others are bedridden and unable to work (Komaroff and Lipkin, 2023).
Common Mechanisms of Action
The COVID-19 pandemic has generated interest in virally associated fatigue syndromes, though not all fatigue syndromes result from viral pandemics. The Epstein-Barr virus (EBV) is the most common cause of infectious mononucleosis and has been the most researched source of postviral fatigue. There is evidence indicating the onset of ME/CFS following viral infections such as EBV, Q fever, influenza, and other coronaviruses (Sasso et al., 2022).
Although SARS-CoV-2 infection has received attention as a potential infectious trigger for ME/CFS (Sasso et al., 2022), additional research is needed to confirm this hypothesis. Indeed, the underlying pathomechanism of ME/CFS also remains unknown because of the multitude of symptoms, including cognitive, endocrine, gastrointestinal, and cardiovascular dysfunction.
FM is a complex disease with uncertain etiology and pathophysiology; however, symptom worsening has been reported following infectious triggers, including SARS-CoV-2 (Attal et al., 2021; Clauw et al., 2020; Fialho et al., 2023). Approximately 30 percent of individuals with FM report physical or psychological triggers prior to disease onset (Fitzcharles et al., 2021). Viral infections linked with FM include hepatitis C virus, HIV, parvovirus, and EBV (Buskila et al., 2008). Lyme disease also has overlapping features with FM, contributing to diagnostic confusion.
“The significant overlap in clinical presentation between Long Covid and ME/CFS and FM raises the question of common mechanisms that could be involved in the pathogenesis of these conditions and offers the potential to use past clinical and biomedical research to accelerate the understanding of pathomechanisms specific to Long Covid.”
Summary and Conclusions
Long Covid shares many features with other complex multisystem conditions. This review focused on similarities with ME/CFS and FM. Other less researched similar conditions include, but are not limited to, POTS, posttreatment Lyme disease, and hypermobile Ehlers-Danlos syndrome. More research is needed to understand infection-associated chronic illnesses.
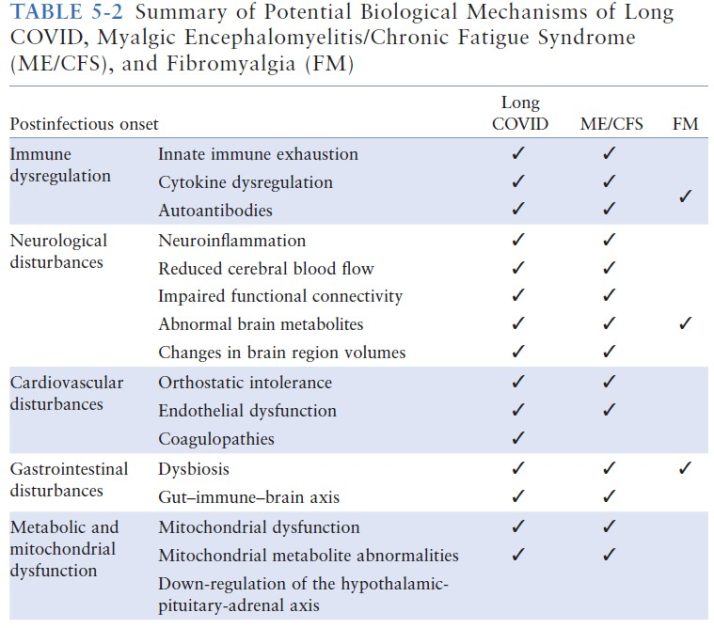
The mechanism of action for these conditions remains unclear, and further investigation is needed. Current theories for potential shared mechanisms of action supported by published literature include:
- immune dysregulation (including dysregulation of innate immune responses, cytokine dysregulation, or mast cell activation);
- neurological disturbances (neuroinflammation has been suggested in ME/CFS and Long Covid);
- cardiovascular damage (endothelial dysfunction, coagulation issues, and orthostatic intolerance have been reported in some patients with Long Covid, ME/CFS, and FM);
- gastrointestinal symptoms (due to gut microbiome dysbiosis);
- metabolic issues (energy insufficiency, reactive oxygen species production, and mitochondrialdysfunction are shared features in Long Covid, ME/CFS, and FM); and,
- genetic variations.
Prognosis
Studies have compared the prognosis and progression of Long Covid and ME/CFS. It appears that in general, Long Covid (especially for Long Covid that does not meet ME/CFS criteria) has a better prognosis than ME/CFS, with some manifestations of Long Covid being similar to those of ME/CFS.
Like ME/CFS, Long Covid appears to be a chronic illness, with few patients achieving full remission. Studies comparing Long Covid and ME/CFS have several limitations, however. First, Long Covid is a new disease, so that Long Covid study participants are usually newly diagnosed, while ME/CFS study participants often have had the condition for a longer time and so are less likely to improve.
Additionally, to qualify for a diagnosis of ME/CFS, symptoms need to be ongoing for 6 months or more, whereas the criteria for Long Covid vary in the literature from 2 to 6 months. Thus, the two conditions are difficult to compare. The full recovery duration for Long Covid patients remains uncertain, but early diagnosis and treatment may help prevent progression to chronic conditions such as ME/CFS and FM.
Treatment
Currently there are no FDA approved drugs or evidence-based treatments for Long Covid, ME/CFS, or FM. The primary approach to managing the three conditions involves the use of techniques, such as pacing and rehabilitation, to manage symptoms and improve functional ability. However, this approach is complicated by multisystem clinical presentation, and treatment approaches may need to be tailored to the individual.
Numerous randomized controlled trials are currently under way to determine the efficacy of a number of identified pharmacological agents; however, limited data have been published, and these trials have yet to be finalized. Moreover, the use of some pharmacological agents is not supported by current research because of the limited understanding of the pathomechanism of Long Covid.
Please note: This is an American report and that here in the UK the NICE Guideline on ME/CFS recommends that ME/CFS can be suspected at 6 weeks of symptoms developing and diagnosed at 3 months. In America, ME/CFS is diagnosed at 6 months. The NICE Rapid Guideline on Long Covid, recommends that Long Covid can be diagnosed if symptoms have not resolved within 3 months of the triggering Covid-19 infection. The Rapid Guideline continues to be updated as the evidence-base develops.